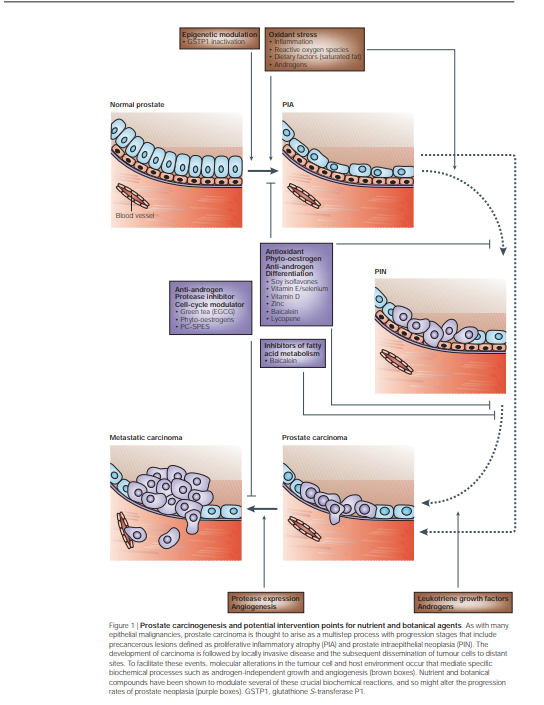
UNCONVENTIONAL THERAPY FOR PROSTATE CANCER: GOOD, BAD OR QUESTIONABLE?
The use of CAM for the treatment of malignant disease is common, and a broad array of vitamins, dietary supplements and botanical preparations are used in this context as an alternative to conventional medical treatments. For this discussion, we define conventional medical treatments as those approaches that are widely accepted and practiced by the mainstream Western medical community. Complementary medical therapies are used alongside conventional medicine and examples include aromatherapy, mental imagery and massage. Alternative medical therapies are used in place of conventional medicine and include homeopathic and naturopathic medicine. Clinicians and patients often use the terms ‘complementary’ and ‘alternative’ interchangeably. Some agents, particularly vitamins, dietary supplements and botanical preparations are used in both contexts. Of the many cancers that affect the population, prostate cancer shows several attributes that provide attractive intervention points for the application of CAMs. The disease is extremely common — with more than 220,000 new cases diagnosed annually in the United States alone1 — and these numbers are projected to increase annually as the ageing population expands. Although specific initiating factors are poorly understood, family history, race and diet are well-documented contributors to risk. Caucasian and African–American men in the United States have a prostate cancer incidence that is 5–50 times greater than that of Japanese men residing in Japan, and the incidence of prostate cancer in Japanese immigrants to the United States is four times that of their native Japanese counterparts. This marked racial and cultural disparity indicates that dietary factors might affect cancer growth. Most prostate cancers initially require the presence of circulating androgens that influence the proliferation and maintenance of the secretory prostate epithelium. Molecular studies also indicate that chronic inflammation might mediate early instigating events in prostate carcinogenesis (BOX 1). Because cell turnover in the prostate is relatively slow, the multistep evolution from an initiated epithelial cell to invasive cancer is estimated to span decades (FIG. 1). This long latency period affords opportunities for intervention with therapies that are designed to delay disease initiation or progression. The standard of care options for treating clinically localized disease include radiation therapies and radical prostatectomy. For advanced disease, ablating androgenic hormones is the mainstay of therapy, and will result in tumour responses in 80–90% of men.